Coronary heart disease, or more accurately, coronary artery disease, which usually manifests itself as severe pain in the front of the chest, is sometimes referred to as the ‘chest plate.’ It may sometimes present without any symptoms. This condition is commonly referred to as ‘silent heart disease.’ Ischemia refers to the insufficient supply of blood to the heart muscle due to blocked heart arteries, resulting in an inability to meet the heart’s oxygen and energy needs. Silent ischaemia is seen in approximately 20% of patients.
Such patients may live for years without knowing they have heart disease or may have had a heart attack (myocardial infarction) without realising it. Despite significant narrowing of the coronary arteries that supply the heart, the patient does not feel any discomfort, especially chest pain. The deadly quartet, or four horsemen of the apocalypse, consisting of diabetes, high blood pressure (hypertension), high cholesterol (hypercholesterolemia) and smoking, plays an important role in the onset of the disease. The incidence of silent ischaemia increases in men after the age of 45 and in women after menopause. Silent ischaemia is particularly common in elderly patients over the age of 80 and in diabetic patients. Since diabetes causes nerve damage (neuropathy), patients may not feel pain. Other risk groups for silent ischemia include:
1- Individuals with a family history of heart disease and sudden death
2- Patients with chronic kidney failure
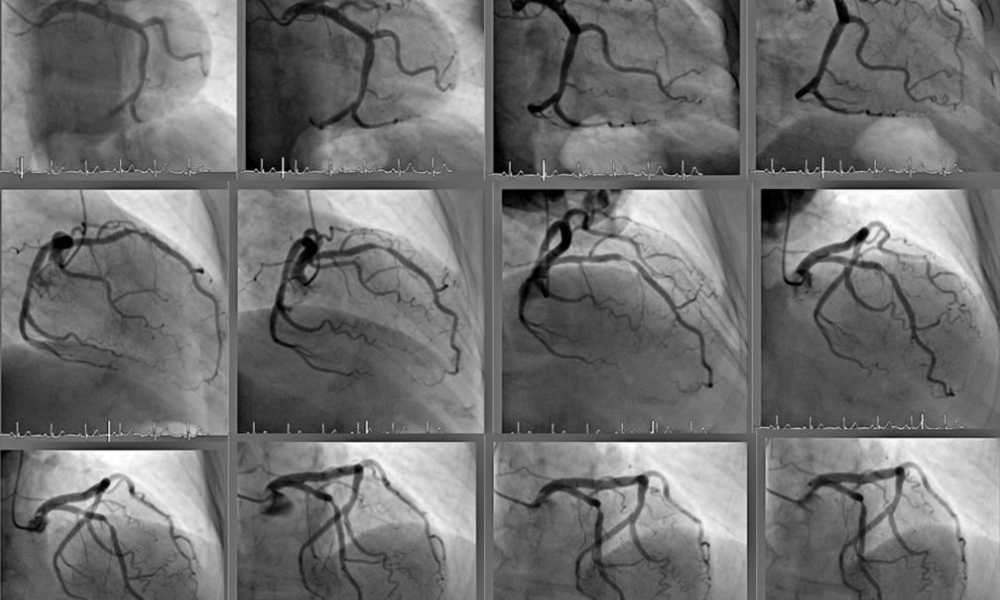
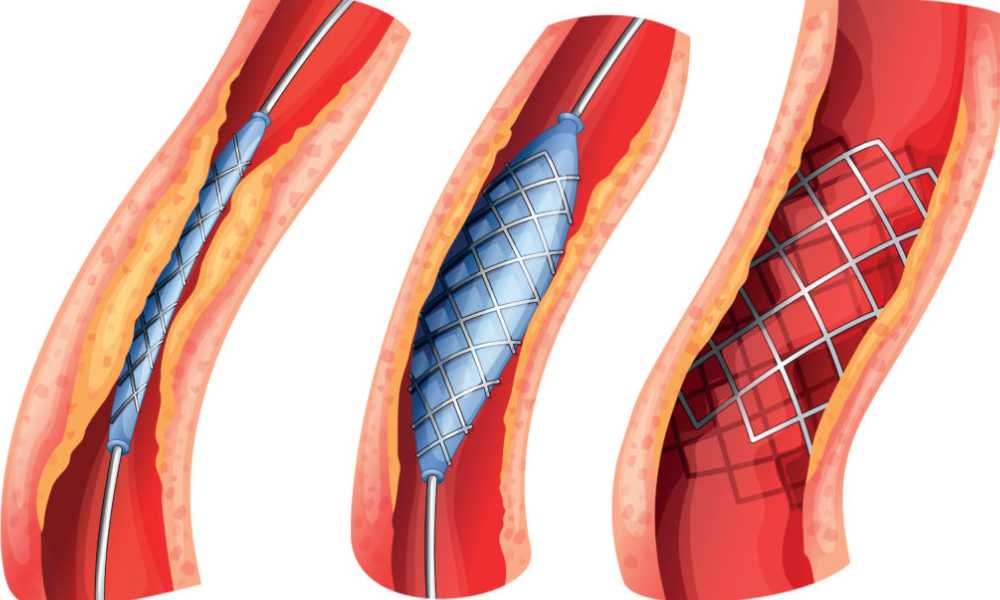
3- Individuals who have previously experienced a heart attack (myocardial infarction) and those with documented coronary artery disease (coronary angiography showing narrowing of the coronary arteries, stent placement, or bypass surgery)
4- Obese individuals
5- Elderly patients who have suffered a stroke
6- Patients with hyperlipidaemia, which is characterised by elevated levels of LDL cholesterol in the blood
7- Patients with a genetic predisposition to blood clotting
8- Patients with chronic obstructive pulmonary disease (COPD)
Coronary artery blockage in the heart, experience chest pain during exertion and are forced to stop and rest, while patients with silent heart disease (silent ischaemia) do not feel chest pain and continue exertion or exercise without resting. This ultimately leads to a heart attack (myocardial infarction). This is because chest pain, which is one of the most common symptoms preceding a heart attack, unfortunately does not occur in these patients. This is the most common cause of heart attacks or sudden death in some people after playing football on artificial turf.
Even if chest pain is not present in these patients, other symptoms such as shortness of breath, dizziness, faintness, nausea, vomiting, fatigue, weakness, indigestion, sweating, and a feeling of suffocation may be present. In situations of mental stress such as excessive sadness, anger, excessive excitement, fear and anxiety, even without exertion, the heart rate may increase beyond our control while at rest, causing silent heart disease (silent ischaemia) to emerge and a heart attack to occur.
The best indicator (marker, indicator) of silent heart disease is cholesterol levels. High LDL cholesterol (bad cholesterol) or low HDL cholesterol (good cholesterol) or both together. In such cases, if other risk factors, family history, or genetic predisposition are present, it is essential to investigate whether the coronary arteries supplying the heart are blocked using other tests. The simplest and most affordable laboratory test to detect silent ischaemia is a 12-lead electrocardiogram (ECG).








 Türkçe
Türkçe